The Strategic Landscape of Epilepsy Treatment
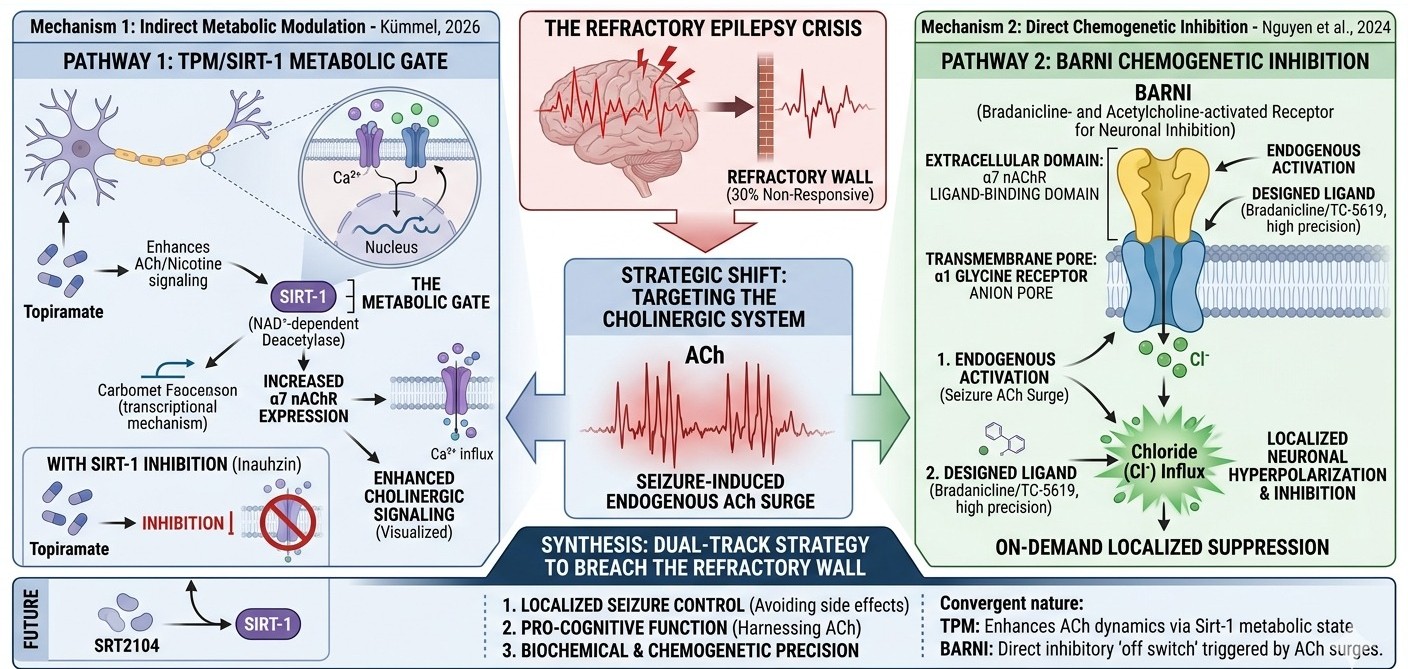
The current trajectory of epilepsy management has encountered a formidable "refractory wall." Despite the accelerated expansion of the neuropharmacological pharmacopeia, approximately one-third of the 50 million individuals worldwide suffering from epilepsy remain resistant to conventional interventions. This clinical crisis stems largely from the limitations of systemic medications, which rely on the broad, often indiscriminate suppression of neuronal activity, inevitably resulting in a high burden of cognitive and behavioral side effects. To break this impasse, a strategic pivot toward the "cholinergic system", a traditionally under-explored territory in antiepileptic drug (AED) design, is now a scientific imperative.
Acetylcholine (ACh), the second most abundant excitatory neurotransmitter in the human brain, is the primary orchestrator of arousal, attention, and memory formation. Its strategic relevance is underscored by the genetic architecture of specific epilepsies, such as Autosomal Dominant Sleep-Related Hypermotor Epilepsy (ADSHE) and Juvenile Myoclonic Epilepsy (JME), which are directly linked to gain-of-function mutations in nicotinic acetylcholine receptors (nAChRs). While ACh is known to regulate the delicate balance of GABAergic and glutamatergic release, the precise biochemical mechanisms by which established second-generation AEDs interact with this system have remained a profound molecular mystery.
Deconstructing the Topiramate Paradox
Unlocking the next era of precision neuropharmacology requires a forensic deconstruction of how "traditional" drugs like Topiramate (TPM) interact with the nicotinic system. Historically, TPM has been categorized by its modulation of GABA and Glutamate receptors; however, the findings of Kümmel (2026) reveal a strategically significant interaction that challenges the established inhibitory orthodoxy.
Utilizing human SH-SY5Y neuroblastoma cells—which natively express a diverse suite of nAChR subunits, Kümmel demonstrated that TPM treatment paradoxically enhances signals induced by both ACh and nicotine. This enhancement represents a radical departure from the profile of first-generation AEDs like carbamazepine and lamotrigine. While those agents were primarily designed to target sodium channels and only incidentally inhibit nAChRs, TPM acts as a unique modulator of the nicotinic signaling cascade.
This discovery redefines TPM as more than a simple inhibitor; it is a metabolic signal enhancer. By augmenting rather than suppressing nicotinic-mediated calcium dynamics, TPM operates outside the "suppression-only" mindset of earlier AED design. This suggests that TPM’s clinical efficacy may be partially derived from its ability to harness, rather than blunt, cholinergic signaling, provided the underlying molecular "master switch" is active.
The Sirt-1 Regulatory Axis: The Molecular Pivot of TPM Activity
The strategic importance of protein deacetylases, specifically Sirtuin-1 (Sirt-1), lies in their role as sensors of cellular energy and regulators of neuronal excitability. As an NAD+-dependent deacetylase, Sirt-1 translates fluctuations in metabolic state into functional changes in neuronal architecture and protection.
Kümmel’s 2026 research identifies Sirt-1 as the critical molecular pivot upon which TPM’s activity depends. The study revealed that TPM’s ability to enhance cholinergic signals is not an intrinsic property of the drug-receptor interaction but is contingent upon Sirt-1 activity. When the specific Sirt-1 inhibitor inauhzin was introduced, the TPM effect was not merely abolished; it was flipped into an inhibitory response. This suggests that the energy-sensing state of the cell acts as a "metabolic gate" for drug efficacy. Furthermore, Sirt-1 is known to increase the expression of the alpha7 nAChR subunit, providing a transcriptional mechanism for this potentiation.
Beyond Traditional AEDs: The Chemogenetic Innovation of BARNI
The strategic shift from systemic pharmacology to targeted neuronal inhibition has culminated in the development of engineered ligand-gated ion channels (eLGICs). The premier example is BARNI (Bradanicline- and Acetylcholine-activated Receptor for Neuronal Inhibition), a chimeric masterpiece of molecular architecture designed to convert excitatory neurotransmission into inhibitory control.
BARNI fuses the ligand-binding domain of the \alpha7 nAChR with the anion-permeable pore of the alpha1 glycine receptor. Unlike traditional receptors that favor sodium or calcium, BARNI opens a chloride-permeable pore upon activation, hyperpolarizing the neuron. Its designer ligand, bradanicline (TC-5619), exhibits a 1000-fold greater affinity for the alpha7 subtype over the alpha4 beta2 subtype, ensuring a level of pharmacological precision that is impossible with systemic AEDs.
A breakthrough realization in this research, enabled by genetically encoded iAChSnFr sensors, is that seizures trigger massive endogenous surges of ACh in the brain. Because BARNI maintains its sensitivity to natural ACh, it functions as an "on-demand" therapeutic regulator. It senses the "temporal spike" of a seizure’s onset and immediately activates its inhibitory pore, providing localized suppression exactly when and where it is required.
This bioengineered precision mirrors the biochemical insights from the TPM/Sirt-1 axis, as both pathways converge on the same temporal surges of neurotransmitter release.
A New Paradigm for Second-Generation Anticonvulsants
The Kümmel 2026 findings and the BARNI research collectively "unmask" the nicotinic system as a central pillar of seizure control, redefining it from a simple neurotransmission pathway into a sophisticated therapeutic target. We are observing a convergence of two distinct strategies. TPM represents an "indirect" modulation, utilizing the Sirt-1 axis to enhance and refine cholinergic signaling according to the cell's metabolic state. In contrast, BARNI provides "direct" inhibitory control, using the same cholinergic surges as a trigger for a chloride-driven "off switch."
Both interventions exploit the massive surges of ACh visualized during seizures. While TPM enhances the dynamics of these surges to potentially trigger neuroprotective Sirt-1 pathways, BARNI utilizes them for immediate hyperpolarization. This represents a tectonic shift toward a "cholinergic-centric" view of neuroprotection.
The Future of Targeted Neuropharmacology
The strategic integration of Sirt-1 and nAChR modulation marks the dawn of a new generation of epilepsy treatments. The clinical potential of this axis is immense, particularly with the advent of highly specific SIRT1 activators like SRT2104. This small molecule is 1,000 times more effective than resveratrol, possesses an absolute bioavailability of approximately 14%, and is already advancing through Phase 2 clinical trials.
As a future adjunct to drugs like TPM, SIRT1 activators could optimize the cellular environment for AED efficacy, ensuring that the metabolic gating remains open for maximal therapeutic effect. These cellular insights pave the way for a dual-track strategy: treatments that are not merely "anti-seizure" but are "pro-cognitive," highly localized, and capable of finally breaching the refractory wall through the marriage of biochemical refinement and chemogenetic precision.


Discussion