Glucagon-like peptide-1 (GLP-1), a naturally occurring incretin gut hormone, regulates blood glucose levels and metabolic function by stimulating insulin secretion, suppressing glucagon secretion, and delaying gastric emptying when blood glucose spikes. However, natural GLP-1 is degraded almost instantly by the DPP-4 enzyme. To overcome this limitation and help patients with chronic hyperglycemia, researchers bioengineered GLP-1 receptor agonists (GLP-1RAs) to mimic the natural hormone while resisting DPP-4 degradation.
Initially, this drug class was strictly recognised as a treatment for Type 2 Diabetes Mellitus (T2DM). More recently, however, it has demonstrated profound benefits not only in glycemic control but also in driving significant weight loss.
The impact of GLP-1 receptor agonists extends beyond glycaemic regulation and weight management. Recent evidence demonstrates that GLP-1RAs elicit significant multi-organ effects, notably in Polycystic Ovary Syndrome (now addressed as PMOS), including direct cardioprotective actions, pulmonary improvements in Obstructive Sleep Apnoea (OSA), and benefits for neurological function. Additionally, GLP-1RAs modulate immune responses by acting on macrophages and T lymphocytes, attenuating chronic systemic inflammation and mitigating immune-mediated tissue injury.
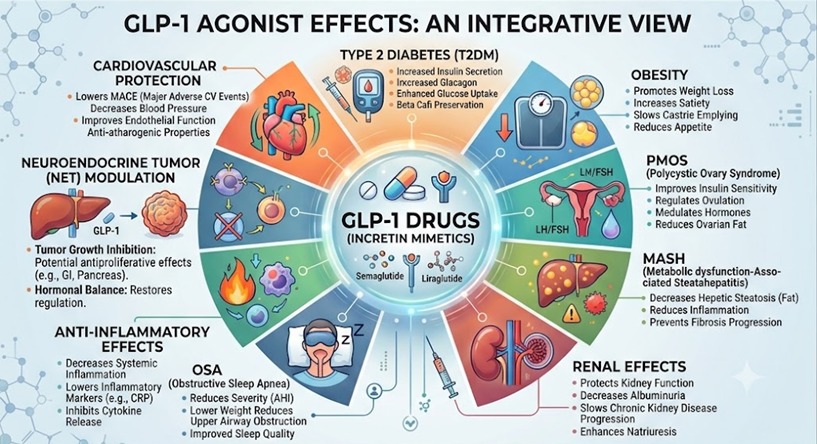
This widespread therapeutic reach is entirely due to the presence of GLP-1 receptors expressed throughout the human body. When activated, these receptors initiate a cascade of protective cellular reactions across multiple vital organs. For this reason, these medications are no longer just diabetes or weight-loss drugs; they are truly a multisystem shield.
Anatomical Mapping of GLP1 Receptors
To understand how this multisystem shield operates, its clinical efficacy must be mapped directly to the precise cellular distribution of the GLP-1 receptor (GLP-1R), a family B1 G-protein-coupled receptor. Vigorous tissue mapping, autoradiography, and mRNA sequencing have shown that the GLP-1R expression extends far beyond pancreatic β cells and embeds itself deeply within peripheral organs, vascular networks, reproductive axes, and the central nervous system.
Pancreatic β-Cell Kinetic Restoration in T2DM
The primary effect of GLP-1 drugs is produced in the endocrine pancreas, where GLP-1R is highly expressed on the surface of islet β-cells. In the setting of Type 2 Diabetes Mellitus, chronic hyperglycemia causes β-cell exhaustion and glucose blindness.
Upon agonist binding, an intracellular cascade triggers the closure of potassium channels and the opening of calcium channels. This precise molecular shift forces high-volume, glucose-dependent insulin secretion, meaning insulin is released strictly when circulating blood glucose is elevated, virtually eliminating the risk of clinical hypoglycaemia.
Concurrently, the drug binds to receptors on pancreatic α-cells, signalling them to shut down the inappropriate overproduction of glucagon. This dual action lowers hepatic glucose output and stabilizes HbA1c levels.
The Brain and Gut Control Centre, Mechanisms of Clinical Obesity Management
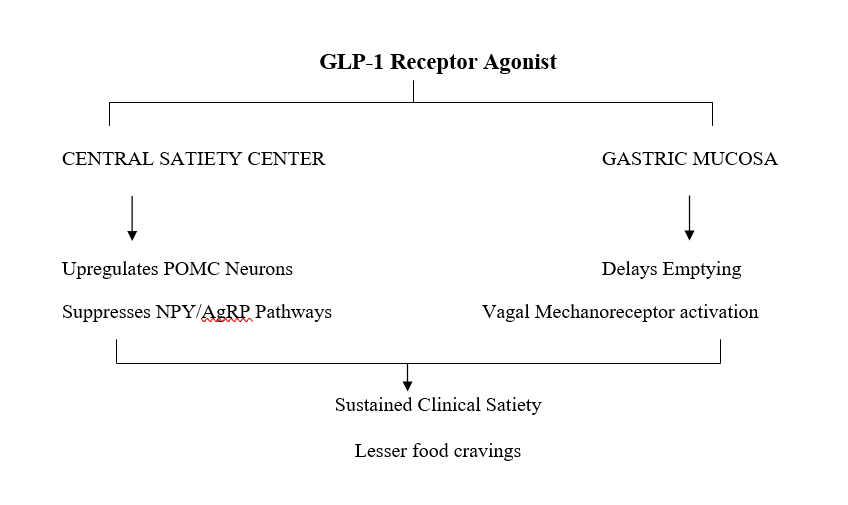
To drive profound weight loss and reverse chronic adipose tissue dysfunction, these agents interface directly with the homeostatic centres of the central nervous system. Receptors are highly concentrated within the arcuate nucleus of the hypothalamus and the nucleus of the solitary tract (NTS) within the brainstem. Within these centres, your brain has two competing sets of signals: one that screams “I'm full” (POMC neurons) and another that screams “I'm starving” (NPY/AgRP neurons).
Because of how these drugs are engineered, they can enter the brain and flip these switches simultaneously, turning up the fullness signals and completely turning down the hunger signals. This shuts off constant, intrusive cravings, which people call “food noise”.
At the same time, the drug acts on your stomach to slow down digestion. Because food stays in your stomach longer, it stretches the stomach wall. This stretching sends a continuous “I am stretched and full” signal up a major nerve (the vagal nerve) straight back to your brain, keeping you feeling satisfied for hours after a meal.
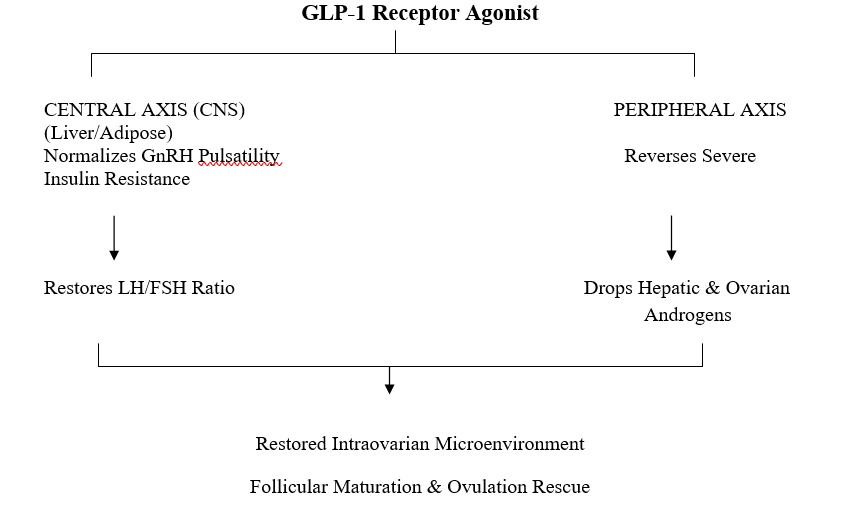
The Reproductive Axis: Rescuing the Neuroendocrine-Ovarian Circuit in PMOS
The drug's systemic impact extends straight into reproductive endocrinology, particularly for patients managing Polycystic Ovary Syndrome (PCOS), now called PMOS. In this, the feedback loop between the brain and the ovaries is completely disrupted. By binding to hypothalamic receptors, GLP-1 agonists help restore the pulsatility of GnRH, which in turn normalizes the LH-to-FSH ratio. At the same time, the drugs tackle the root metabolic problem by reversing insulin resistance throughout the body. By dropping these chronically high insulin levels, the ovaries are no longer overstimulated into producing excess male hormones like testosterone. This simultaneous central reset and metabolic cleanup lowers total background inflammation and restores a healthy, balanced environment within the ovaries, allowing egg follicles to mature normally and successfully rescuing regular ovulation.
Cardiovascular Remodelling and Endothelial Signalling
Simultaneously, these receptors are densely expressed in vascular endothelium of blood vessels, smooth muscle cells, and the Sinoatrial node (SA node) of the heart. Rather than altering myocardial tissue directly, receptor activation here promotes a cascade of reactions through which nitric oxide (NO) is formed and drives vasodilation, reduces blood pressure, and mechanically stabilises atherosclerotic plaques against rupture by altering their cellular architecture.
Resolving MASH via Hepatic Immune Modulation
While hepatocytes themselves lack significant GLP−1R density, the shield powerfully mitigates Metabolically Dysfunctional-Associated Steatohepatitis (MASH) by targeting the liver’s innate immune architecture. The receptor maps heavily onto circulating monocytes, tissue macrophages, and hepatic Kupffer cells. In the pathogenesis of MASH, these resident macrophages adopt a pro-inflammatory M1 phenotype, driven by the master transcriptional regulator NF-κB.
Upon agonist binding, intracellular signalling cascades inhibit the translocation of NF-kB to the nucleus. This molecular arrest effectively halts the downstream transcription and secretion of destructive pro-inflammatory cytokines, specifically Tumour Necrosis Factor-alpha (TNF−α) and Interleukin-6 (IL−6).By silencing this localised cytokine storm, GLP-1s alleviate the chronic immune-mediated stress inflicted upon adjacent hepatocytes. This interrupts the cycle of lipotoxicity, shielding liver cells from inflammatory apoptosis, suppressing the activation of scar-forming hepatic stellate cells, and ultimately driving the resolution of hepatic steatosis and fibrosis.
Pulmonary Architecture and Renal Hemodynamic
Receptors located within pulmonary smooth muscle lines and renal vascular beds work in tandem with visceral fat loss to manage complex cardio-renal conditions. According to a recent narrative review, GLP-1 receptor agonists may help manage obesity-related obstructive sleep apnoea by promoting weight loss, which can lead to improvements in airway structure and function. The review also discusses their effects on various organ systems, including the kidneys, where they may help reduce glomerular hyperfiltration. This action relieves hydrostatic pressures within the nephron, providing direct microvascular protection that slows the progression of chronic kidney disease.
Immunomodulation and Anti-Inflammatory Effects
The broader systemic efficacy of the GLP-1RA class relies on its role as an immunomodulator. Chronic metabolic diseases lock the body into a state of low-grade, destructive systemic inflammation. GLP-1 agonists act as a metabolic circuit breaker by forcing a critical phenotypic shift in macrophages.
In obesity and T2DM, the immune system is dominated by M1-polarised macrophages, which actively secrete inflammatory markers that damage blood vessels and scar liver tissue. Upon GLP-1R activation, these cells are reprogrammed into M2-polarised macrophages, transitioning the immune response from an aggressive, pro-inflammatory state into an anti-inflammatory, tissue-repairing state. By calming this background immune noise, GLP-1s protect vital organs from progressive fibrotic damage and oxidative stress.
The Oncological Frontier: Receptor Homing and Neuroendocrine Tumours
According to a recent article, GLP-1 receptor agonists are being explored for their potential to protect organs from fibrotic damage and oxidative stress by influencing immune pathways, and they have also emerged as a promising area of research in cancer therapy for their possible anticancer benefits in Neuroendocrine Tumours (NETs). Certain malignancies, particularly benign and malignant insulinomas, gastrinomas, and other gastroenteropancreatic neuroendocrine tumours, express an exceptionally high density of GLP-1 receptors compared to healthy surrounding tissues.
Rather than relying purely on the hormone's metabolic actions, oncologists are utilising the GLP-1R expression profile as a biological homing beacon via Targeted Radionuclide Therapy. By bioengineering GLP-1 receptor agonists fused to radioactive isotopes (such as Indium-111 or Lutetium-177), scientists can inject these compounds intravenously.
The engineered peptide travels through the bloodstream, bypasses healthy tissue, and locks directly onto the high-density GLP-1R cluster on the tumour surface. The cell internalises the receptor-agonist complex, delivering a highly localised, lethal dose of radiation directly to the malignancy while completely sparing healthy surrounding organs.
Conclusion
The evolution of GLP-1 receptor agonists marks a massive shift in how we approach metabolic care. What started as an effort to manage pancreatic insulin has turned into a multi-organ treatment strategy. By mapping onto receptors across the brain, cardiovascular system, and immune cells, these molecules are rewriting the treatment guidelines for interconnected chronic diseases.

Discussion